

Updated March 25, 2020 to Version 1.4
Using This Record
Whether you oversee a microsanctuaryA microsanctuary is a small scale community of human and nonhuman (generally “unconventional or farmed”) animal companions, who live together in a chosen shared lifestyle and in commitment to ending the oppression of all beings. Microsanctuaries adhere to the notion that no nonhuman member of the community should “serve a purpose.” Microsanctuaries can exist in any context: rural, suburban, or urban. A microsanctuary can consist of as small a community as one animal and one human caregiver. For more information on microsanctuary please refer to the Microsanctuary Resource Center. with just a few residents or a large sanctuary with hundreds of residents, keeping track of healthcare treatments and staff observations is important. How you ultimately organize and save that information going forward may look different, but regular use of the Ongoing Treatment and Observation Record (or something similar that you’ve tailored specifically to your needs) will likely be necessary. Any time a resident has a health concern or receives any sort of treatment, this information should be recorded.
While you may think that having many different types of records that each serve a very specific purpose might be helpful, in practice it can sometimes be cumbersome, especially for sanctuaries with larger resident populations. Therefore, we wanted to provide sanctuaries with a document that is versatile. There are many different ways to utilize this record and chances are you may think of a unique way to make it work based on the specifics of your sanctuary. We’ll look at each section of the record and offer some instruction and suggestions for how to make the most of this document.
Header
This one is pretty straightforward. In addition to specifics about the resident, we also offer spaces for:
- Year – This is helpful when compiling a resident’s permanent record, especially if you have a backlog of records.
- Treatment Record Number – In many cases, a resident may have multiple records pertaining to one ongoing treatment. Having them numbered in advance can make recordkeeping easier later on.
Resident Health Alert
This section may not be necessary for every resident, but may come in handy for others. This gives you a place to put important information that staff should know about when working with the resident or administering their treatments. Some information that would be helpful to include here might be:
- Known allergies – “Allergic to chlorhexidine. Use dilute betadine.”
- Contraindicated drugs – “Kidney disease- do not give NSAIDs.”
- Important information about treatment – “Sneaky about spitting out pills! Watch closely to ensure he swallows.”
- Special instructions about restraint – “Heart issues. Do not tip on her side.”
- Reminders – “Call vet with update on Monday” or “Recheck appointment on 4/7.”
Condition(s) Being Treated
This section is used to record the basics of the condition or conditions being treated. Some people find it helpful to number each condition if listing more than one, others find a different way to clearly separate them though the use of bullets, backslashes, or semicolons. You will see in the next section that each treatment listed will be clearly associated with a corresponding condition. Tips for using this section:
- Include all important information – Simply writing down “limp” won’t be as helpful later on as “limp on front right leg associated with CAE.”
- Update the condition based on diagnostic results – At first, the condition might be a bit general (“cyanotic with labored breathing”), but after a veterinary examination or diagnostic results, you may be able to update the condition with more specifics (“cyanotic with labored breathing due to aspergillosis”).
Treatments/ Monitors/ Etc.
There are five numbered sections on this chart. These can be used to list any medications the resident is currently on, other types of treatments (such as a foot wrap or wound treatment), regular health monitors (such as monitoring a healing incision or wound, or rechecking a resident for external parasites), and can also be used to keep track of a new resident’s incoming needs (fecal check, vaccine schedule, neutering, etc.). We’ll look at each of these in more detail below.
Medications
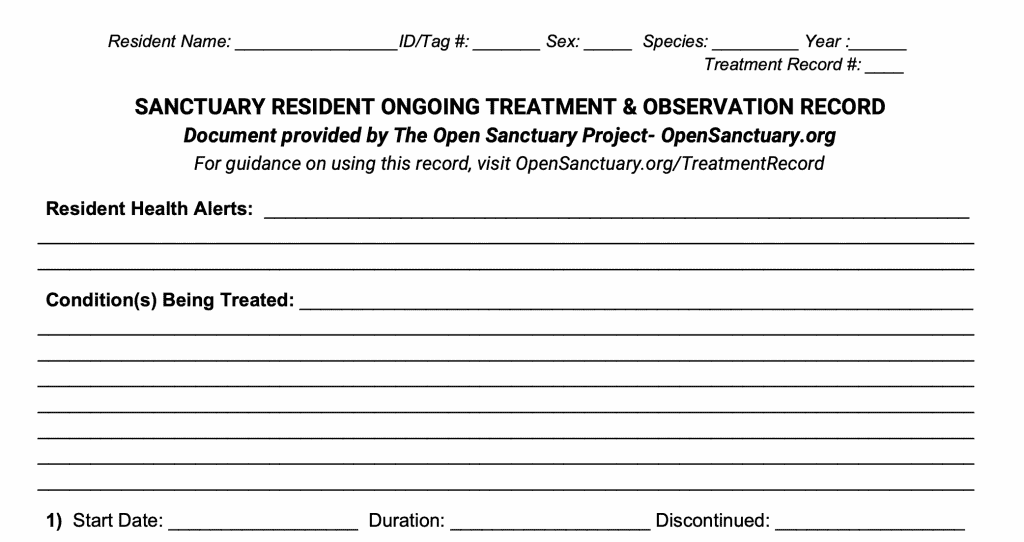
In this example, you can clearly see the date the medication was started as well as the specifics of the treatment. Be sure to include the following information, though you may have a different format you’d like staff to use:
- Drug name (Meloxicam)
- Drug strength (7.5mg)- This information is important because many drugs are available in a variety of strengths. When you refer back to this information, you want to clearly see what strength medication was given. Confusing 7.5mg Meloxicam with 15mg Meloxicam could have dire consequences.
- Dose (½ tab)- For tablets and capsules, this will include the number (including any partial tabs); for oral suspensions and injections, this will include the volume (for example, 1.5ml).
- Route of administration– In this example, the route of administration is not listed because it is implied by the fact that it is a Meloxicam tab. However, you may choose to include the tag “orally” or “PO” just to be clear. Other medications will require more specifics, especially injectable medications in which you will need to clarify if it is given subcutaneously or intramuscularly, and if it needs to be given in a specific location (for example, behind the ear).
- Frequency (2x day)- You may choose to write this differently, but be sure to clearly state how often the medication is being given. In this instance, we do not specify when the medication is given, but if it were given just once a day or once a week, we would need to add more specifics (“once a day in the AM” or “every-other-AM”).
- Duration- In this example, the duration space is left blank because the Meloxicam may go on until symptoms resolve, but in other instances, the treatment may have a clear duration (“10-14 days” or “7 days max”), or you may choose to also include the date to better keep track of the treatment duration (“until April 1-5”).
The bottom line of each numbered section provides a space to clearly connect each treatment with a condition, which comes in handy when dealing with multiple treatments and multiple conditions. You may choose to write in the condition as seen here (“limp”) or you may choose to number each condition and simply place the number in this space, which will be helpful for lengthy conditions. There are also boxes to indicate if this is a:
- New Treatment – Check this box if this treatment is newly started.
- Ongoing Treatment – Check this box if this chart is a continuation from other charts (someone on long-term analgesics may have numerous charts for one ongoing treatment).
- Resumed Treatment – Check this box if this is a treatment that was temporarily discontinued and is now restarted. Perhaps it appeared that a painful limp had resolved on NSAIDs, but after a time off the medication the limp returned and the treatment was resumed, or perhaps a goat resident on Bute was temporarily switched to Banamine because they were especially pained.
- Adjusted Treatment – Check this box if the medication remains the same but the dose, frequency, or administration route has changed. For example, if a resident is doing well on analgesics twice a day, you may decide to see if decreasing the frequency to once a day continues to keep them comfortable. Or, you may find that an oral formulation is not working well and decide to try out the injectable formulation.
This information can be helpful in a few different situations, but is especially helpful when compiling a resident’s permanent record.
Here’s another example:

In this example, the resident is on two treatments for the same condition. The main difference here is that the second medication is an oral suspension, so the dose is in milliliters and the strength is in milligrams per milliliters.
Monitors
This chart can also be used to track health concerns that need to be monitored regularly. These monitors may be in addition to a treatment in some cases, or could be the only item on the chart.

In this first example, the resident is on a monitor for a recurring limp after their Bute treatment was discontinued. This is a good way to assess how a resident is doing post-treatment.
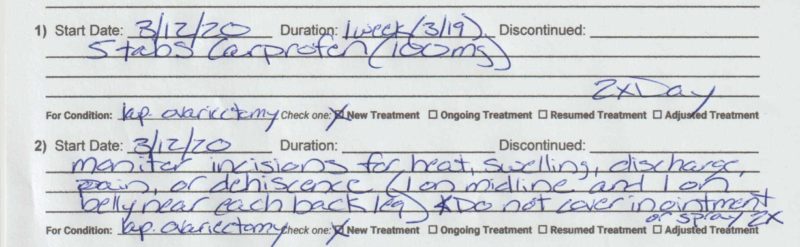
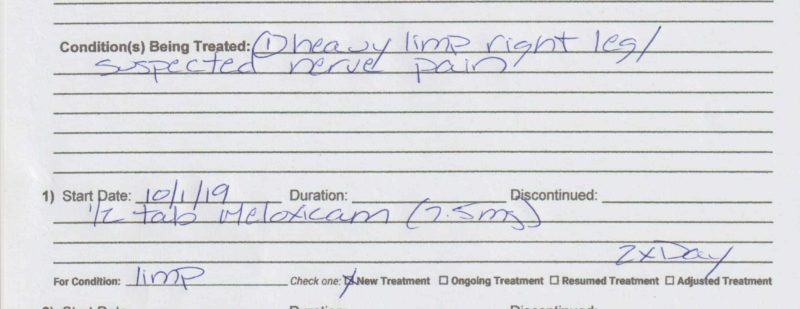
In this example, the resident recently underwent a laparoscopic ovariectomy. In addition to medications, they are also on a monitor of their incisions. (You can also see the “Duration” section in use here since the Carprofen is a short-term treatment).
Discontinuing a Treatment or Monitor
When a treatment or monitor is discontinued for whatever reason, this must be clearly indicated on the treatment record. In some cases, once a treatment is discontinued there will be no reason to continue using the treatment record, but other times, there may be other treatments or monitors on the record that continue. An easy way to indicate that a certain item has been discontinued is to draw a single slash through it, write “D/C” (discontinued), and record the date the treatment ended.
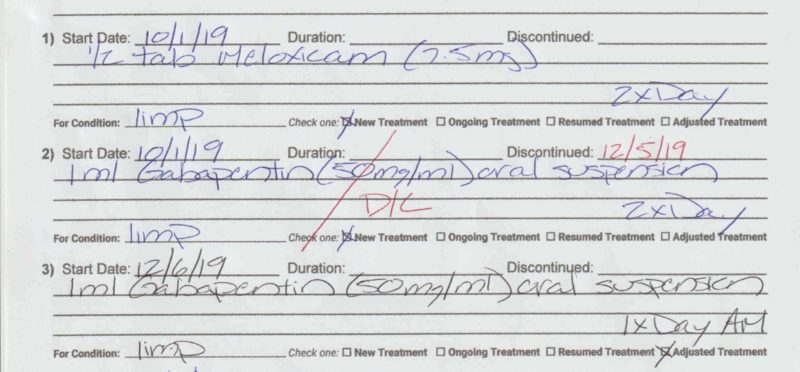
Here you can see the resident was on Meloxicam and Gabapentin twice a day for a limp (remember, more details about the limp will be listed in the “Condition(s) Being Treated” section). The resident is doing well, so their caregivers are working on weaning them off the Gabapentin. When the frequency was reduced to once a day in the morning, the initial Gabapentin treatment was discontinued and the adjusted treatment was added. You may opt to use a different technique to indicate that a treatment has been discontinued. The main thing to keep in mind is that you want to be able to read the information that has been discontinued, so drawing a horizontal line through the entire text would not be recommended.
Incoming Resident Needs
Often, when a new resident arrives, there are many things they require depending on their age, species, and your sanctuary’s incoming protocols. Some of these things take place immediately upon intake, others might be able to wait a few days while the resident gets acclimated, and some things might have to wait until the resident reaches a certain age or until their health improves. It can be difficult to keep track of what has been done versus what still needs done, so it can be helpful to use this record to keep track of everything.

Here you can see the various incoming treatments and procedures the new resident needs. Because of their age, the Triangle 10HB and Rabies vaccines both have a future date indicating the point at which they will be old enough to receive the vaccines.

As the various items are completed, the box is checked and the date is written down. This way, you will have a record not only that each item was completed, but also when the item was completed.
General Species Observations
Depending on the size of your resident population (and possibly the size of your caregiving team) it can be helpful to have general observation records. In most cases, residents will only have a treatment record for current treatments or monitors, but it’s not at all uncommon that you may need to record an observation about a resident who does not have a current treatment record. For example, perhaps you are in with your sheep residents and you see a resident cough twice. They appear to be fine otherwise, have no known health issues, and are in the middle of eating hay. The cough was dry, and they are showing no other signs of respiratory issues. Could it be that they simply inhaled a few small dust or hay particles while eating? Yes. But is it possible this is the start of something? Also, yes. If next week the coughing is worse or they suddenly seem less interested in eating, you will want to be able to tell your veterinarian when you first heard them cough. If an ongoing issue is noted based on observations on this chart, you can then create an individual chart for the resident. Some sanctuaries choose to create a separate document for general observations of this nature, but because it is often easier to have one document that can function in a variety of ways, it may be helpful to use this treatment record as a general observation sheet. To do so, you may leave much of the front of the record blank and simply write “General Sheep Observations” in “Condition(s) Being Treated” or somewhere else on the record to clearly state its purpose. It’s really the back of this record that is most useful for general observations.
Using The Table On The Backside
The table on the back of the record is where most of the action happens. Every time a treatment is administered or a monitor is conducted, the appropriate staff member fills in a row (or more) of the table by initialing the appropriate box and recording their observations.
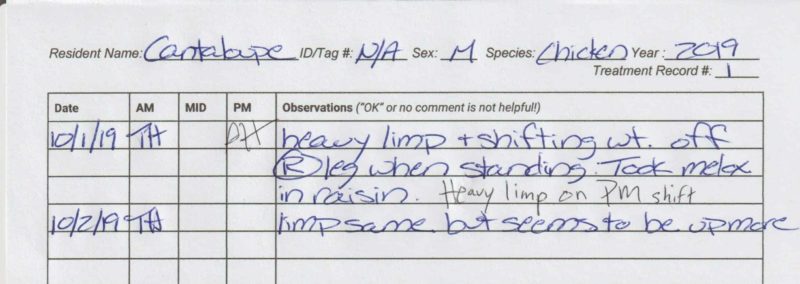
You’ll see the note in the observations column- “OK” or no comment is not helpful! – The observation column is an important tool to track a resident’s progress. It’s important to train people to fill out this section in a way that is useful. Imagine this scenario- Fran is an elderly sheep and is on NSAID treatment for arthritis. One day, while getting ready to clean her indoor living space, a staff member tries to encourage her to stand and walk outside, but she refuses. The staff member tries to help her to stand and realizes that she cannot. You look back through her treatment record to see how she’s been doing the past few days to get a better idea of how she’s been doing lately. In the observation column you see “OK” for the last 5 days. What does this mean? After speaking with the various staff members who administered her medications over those 5 days, you find out that she was bright and excited about her medications but remained lying down each day. After more discussion, you realize she may have been in the same spot for at least the last 3 days. If, instead of writing “OK” staff were more descriptive, you might find something like this instead:
2/7/20- Excited for syringe but remained down.
2/8/20- Laying down next to hay feeder. Bright and eating hay.
2/9/20- Cuddled next to Joan. Still by feeder. Excited for meds.
Hopefully, with notes such as these, staff would realize that Fran has not been seen standing for a few days and seems to be staying in the same spot. Staff could then proactively investigate the situation, perhaps speaking with other staff to see how Fran was during feeding time or simply going out to spend a bit of time with her and see if they can encourage her to stand. While observations regarding their demeanor and location can be very helpful, it’s also important to make sure the condition being treated is being evaluated as well. If Fran is on NSAIDs for a significant limp in her front leg, it’s important to track how she is moving. This can be a bit of a gray area- do you force a resident with mobility issues to stand every time you see them so you can evaluate how they are moving? That may be a bit excessive and cause the resident unnecessary discomfort. You may opt for other ways to gather this information while taking the resident’s comfort into account- perhaps you know their living space is cleaned every-other-day and that all residents are moved outside during this time. You might make a point of having staff evaluate certain residents at this time, being sure to include their observations on the treatment record.
Just as “OK” is not very helpful, neither are certain other comments. If a resident is being treated for a limp, it is not helpful to simply write “limping” everyday. Assessing progress requires detail. Staff should be trained to use descriptors- if most days a resident’s limp is recorded as being “slight,” and suddenly someone sees them with a significant limp or refusing to bear weight on that leg when standing, those are clear changes that would not be obvious if one simply wrote “limping” each day.
In addition to comments about the resident’s specific health status, it is helpful to record observations regarding behavior and social dynamics. For example, if a new resident is very wary of human attention but starts warming up to a certain caregiver or seems to respond well to a specific sort of interaction, these are helpful details to note. Perhaps they are unwilling to approach a human who enters their living space, but are more comfortable approaching a human who is on the other side of a fence. Knowing and documenting this information can help staff create a plan for slowly and gently getting the new resident to become more comfortable. On the other hand, if you know that a certain resident craves human attention and always comes running when caregivers enter their living space, but one day they seem more wary, this is important to note and to investigate. This can also be a helpful way to keep track of residents who are especially bonded or who seem not to get along well. If the resident has their own chart for an ongoing treatment or monitor, this information could be recorded there, or if they do not, it would go on the general species observation record.
Overall Assessment
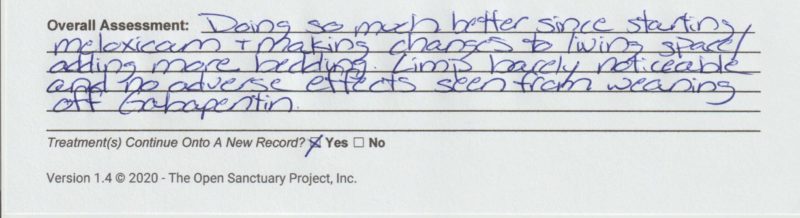
When a treatment record is complete (either because all treatments/ monitors have been discontinued or because there are no more empty rows in the table) a staff member should write a brief summary of how the resident is doing based on the recorded observations. Who fills this out may vary by sanctuary- perhaps whoever completes the table or discontinues the items on the front side is responsible for writing the overall assessment. If your sanctuary has certain staff who oversee resident care, such as a species specialist or caregiving manager, they may be the person responsible for completing this section, and the act of filling it out can be a great way for these people to check in on the residents they are responsible for and take some time focused on their progress. Staff will also indicate if the resident’s treatments continue onto a new record or not.
A Few Other Notes About Using The Treatment Record
Different sanctuaries will have different variations of how they use this treatment record depending on the other systems they have in place. For example, at smaller sanctuaries, the treatment records may be the sole way that information related to treatments is communicated, whereas at larger sanctuaries there are often other systems in place used in conjunction with the treatment records. If the treatment record is the sole way treatment information is communicated, it may be helpful to include a few other details such as:
- Location – If your sanctuary has multiple living spaces, it can be helpful to indicate where the resident lives. This may seem unnecessary, especially if your sanctuary has only a few residents and only one or two caregivers, but it can come in handy in the event that a volunteer or other staff member has to step in unexpectedly. Some sanctuaries have systems in place to look up where a resident lives- this may be a database that includes their location or even a white board that lists the residents living in each area. If your sanctuary has a system in place to easily figure out where everyone lives, you won’t need to include this information on their treatment record.
- Additional Identifier – If all of your chicken residents have leg bands, this can be a useful way for people to communicate about a resident whose name they have not yet learned. They may see someone limping and be able to look at their leg band and communicate that “Yellow 95” was limping, to which staff can respond “That’s Penelope.” However, if a person is tasked with finding Penelope by being told she has a yellow 95 tag, that can be a bit more difficult. It may be easier to identify Penelope by looking for “the only white hen with black speckles on her back.” Again, this may not be necessary for regular caregivers but can be useful in the event someone else needs to step in. Some sanctuaries have other systems to identify residents such as a database with names and descriptions or even simply a binder of alphabetized photos. If you have a system like this in place, including this information on the treatment record is likely unnecessary.
- Additional details about how to administer treatment – If your sheep residents typically receive their oral medications in a syringe full of molasses, but Apollo will only take his medications in applesauce, you will likely want to have this information somewhere so caregivers know how to prepare his syringe. Some sanctuaries have systems in place to prepare medications in advance and may use labeled ziplock bags or bins to keep everything organized. If this is the case, the information about how to prepare Apollo’s syringe would likely be on his labeled bag and would not need to be on his record (though you should probably make a note somewhere that he prefers applesauce in case he needs oral medications again in the future).
- Color-Coding Treatment Records – Depending on the number of treatment records being used at any given time, it may be helpful to use different color paper to distinguish between different types of records. For example, you may choose to print a set of records on purple paper and use these for general species observations, which can make them easier to find and organize. Sanctuaries with large resident populations might find it useful to use different colored paper to differentiate between treatments or monitors that happen once a day versus those that are done more frequently. If you set up resident treatments so that all once daily treatments/ monitors happen earlier in the day, having twice daily (or more frequent) records in a different color can make signing off on records at the end of the day easier because staff can quickly flip through to the appropriate records by looking for the corresponding color.
What Should Be Done With Completed Treatment Charts?
This record is just one part of the recordkeeping process. Utilizing it regularly is the first step. Next you need a system in place to access this information in the future. The size of your resident population will likely impact what that system ultimately looks like. If you care for a small flock of chickens with no plans to expand, you may choose to file these treatment records as they are in a resident’s permanent file (which may be an actual file of papers, or perhaps a binder). Others may choose to scan these records and create digital folders for each resident. For sanctuaries with a large number of residents, especially those who have been around for some time, these systems may be too cumbersome and make retrieval of information difficult. In these cases it may be best to take these records and compile the information into one larger ongoing record. You’ll have to figure out what makes the most sense for your sanctuary; just make sure that if you need to look back and find information (even from the record of a resident who is no longer at the sanctuary) that you are able to do so fairly quickly and easily. You may not know it at the time, but this condition you are treating Walter goose for may end up being a recurring issue. When it resurfaces, you’ll want to be able to look back through his record to see when the issue happened originally, how long it lasted, and how he responded to treatment. Or perhaps one of your residents has an uncommon issue that you know Matilda had 6 years ago. You’ll want to be able look through her record to find information about effective treatments. There are various advantages to maintaining an online recordkeeping system rather than, or in addition to, a paper record. For more information about recordkeeping, including a link to a free and secure online recordkeeping system, check out our resource here.
Download The Ongoing Treatment And Observation Record
Enter either your organization’s name or your name and email below to download a free printable double-sided form to help keep track of regular treatments and observations for sanctuary residents, either as part of ongoing care, quarantineThe policy or space in which an individual is separately housed away from others as a preventative measure to protect other residents from potentially contagious health conditions, such as in the case of new residents or residents who may have been exposed to certain diseases., or for a variety of other purposes! Check out our resource here to learn more about the importance of sanctuary resident recordkeeping!
Looking for a form more suited to longterm care documentation, such as vaccinations, hoof trimming, and more? Check out our Longterm Treatment & Care Record!
We promise not to use your email for any marketing purposes! Would you prefer to access this form in a different way? Contact us and let us know!


